In summary
siRNA drugs work very similarly to ASOs, because siRNA drugs ultimately prevent the “bad gene” from being translated. The siRNA drug mechanism is more complex though, because it starts as a double stranded RNA (dsRNA) molecule that undergoes several processing events by endo-ribonucleases to not only shorten the siRNA sequence but also to create a single stranded RNA (ssRNA) molecule from the original dsRNA molecule.
In depth
Last month, I went over how gene silencing drugs work using ASOs as an example, so feel free to reference that if you’re a little confused! Now, RNA interference (RNAi) technology is a pretty hot topic in gene therapy lately, and there’re a few different flavors–our friend, siRNA, is a more prominent modality, but we also have micro RNA (miRNA) and small-hairpin RNA (shRNA) that ultimately interfere with the RNA translation process in the body. And I’ll stick with siRNA today, but perhaps I’ll write a post in the future talking about the differences between these three if anyone is interested.
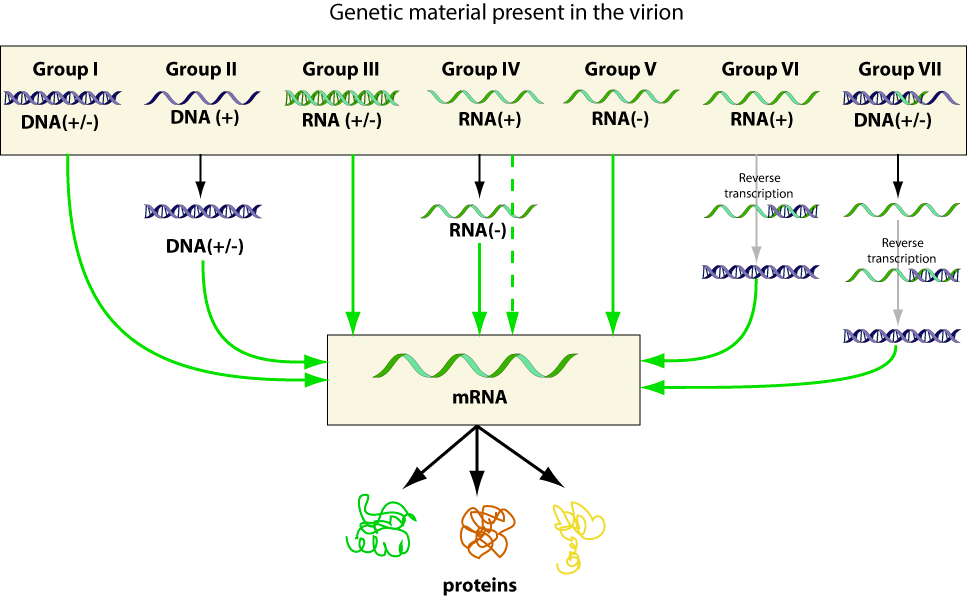
Now, let’s start with the dsRNA structure, because this is very unique. To do this, let’s go into some basic virology. dsRNA is not a common structure for human genetic information–DNA is double stranded, and RNA is single stranded, but dsRNA is abnormal. Now, when the body sees a foreign dsRNA molecule, it triggers an innate immune response, because it sees the dsRNA structure and thinks “virus!” Look at the picture below, and you can see that there’s a whole group of viruses (Group 3) that passes genetic information along in dsRNA form:
Now, a good question is why are these drugs double stranded if that’s going to cause an innate immune response? One reason could be that dsRNA is much more stable than ssRNA. Another reason could be because DICER, our first protein type of the day, needs a dsRNA molecule to start the first series of siRNA processing events. One of the differences that I’ve noticed is that siRNA drugs differ from ASOs because siRNA drugs almost seem like prodrugs–they need a little more processing by these enzymes in the body to become functional, where as ASOs are pretty much ready to work as soon as they find their target site. And I’m sure there’re pros and cons to each, but let’s move onto the next stage.
Thanks to our friend, DICER, that cleaved the irrelevant pieces of our siRNA drug, we now have a shortened, but still dsRNA molecule. Since the siRNA molecule has been shortened to around ASO length (~20 base pairs), the siRNA molecule interacts with our second protein type of the day, the Argonaute proteins. The Argonaute proteins have a cool name because one of the proteins looks like an octopus, Argonauta argo! Once the dsRNA molecule forms an RNA-Induced Silencing Complex (RISC) with the Argonaute proteins, the siRNA is converted to a ssRNA molecule via an unwinding procedure. Now that there’re 2 strands of ssRNA, each is given a name. The unused strand of ssRNA is called the passenger strand, and it’ll be immediately degraded by the RISC. The ssRNA strand that does all the work is called the guide strand, and that strand will attach to the mRNA strand of the “bad gene.” Once the guide RNA strand binds to the mRNA strand, the RISC recognizes the siRNA-mRNA complex and cleaves the mRNA, rendering it untranslatable. The mRNA is then further degraded by cellular enzymes, as if it never existed.
Just like in ASOs, siRNA doesn’t solve the root problem of why the gene is failing, so it must be continually administered for therapeutic effect. However, I actually found this one paper that explains how siRNAs are more efficacious at gene expression inhibition than ASOs. Like this other paper explains, siRNA is technically less complicated in the body as well, because the mechanism is more like fitting puzzle pieces together than having to fit a million keys into a specific lock, which could add to the efficaciousness of RNAi as opposed to protein gene therapy modalities.
In literature
These are some of my favorite papers to help you learn more about siRNAs!
https://pubmed.ncbi.nlm.nih.gov/34044011/
https://pubmed.ncbi.nlm.nih.gov/22737048/
https://pubmed.ncbi.nlm.nih.gov/33513339/
Next month, let’s talk about a different type of modality, peptide gene therapy.

One thought on “How do small interfering/short interfering/silencing RNA (siRNA) gene therapy drugs work?”